Plans are steering employees toward expanded telehealth options and high-value centers of excellence
By Stephen Miller, CEBS
August 13, 2018 - SHRM
With the cost of employer-sponsored health care benefits expected to approach $15,000 per employee next year, large U.S. employers continue to make changes, new research reveals.
Many want to hold down cost increases and are steering employees toward
cost-effective service providers, such as telehealth options and high-value
in-plan provider networks, according to the nonprofit National Business Group on
Health (NBGH) survey 2019 Large Employers' Health Care Strategy and Plan Design.
The survey was conducted from May to June with 170 large employers as they
finalized their 2019 health plan choices; more than 60 percent of respondents
belong to the Fortune 500.
Big employers project that their total cost of providing medical and pharmacy benefits will rise 5 percent for the sixth consecutive year in 2019. If they weren't making benefit changes, their costs would rise 6 percent, the survey showed.
The total cost of health care, including premiums and out-of-pocket costs for employees and dependents, is estimated to average $14,800 per employee in 2019, up from $14,099 this year. Large employers will cover roughly 70 percent of those costs, leaving $4,400 on average for employees to pick up in premium contributions and out-of-pocket expenses.
Health benefit costs are still rising at two times the rate of wage increases and three times general inflation, "making this [cost] trend unaffordable and unsustainable over the long term," Brian Marcotte, NBGH president and CEO, said at an Aug. 7 press conference in Washington, D.C.
"The most unexpected data point in the survey this year is that employers are dialing back their move to consumer-directed health plans"―or CDHPs―especially as a full replacement for other health plan options, Marcotte said. CDHPs typically combine a high-deductible health insurance plan with a tax-advantaged account that employees can use to pay for medical expenses, most commonly a health savings account (HSA) or health reimbursement arrangement.
"We may be at a tipping point in terms of cost-sharing with employees," Marcotte said.
In 2019, the number of employers offering CDHPs as a sole option will drop by 9 percent, from 39 percent to 30 percent, "reflecting a move by employers to add more choice back into the mix" by also offering traditional health plans such as preferred-provider organizations, he noted.
To lessen the pain of high deductibles while maintaining incentives for
cost-conscious spending, large employers are contributing to their employees'
HSAs, on average, $500 for an individual and $2,000 for a family, NBGH
found.
The shift to CDHPs as a sole option over the last decade was driven, in
part, by the Affordable Care Act and its 40 percent "Cadillac tax" on high-value
health plans, originally to take effect in 2018, Marcotte said. "A lot of
companies moved to high-deductible health plans to minimize the impact of the
Cadillac tax or to delay its impact, but the Cadillac tax has been kicked down
the road, first to 2020 and now to 2022," Marcotte said. Many believe it may be
further delayed or repealed altogether, "so employers are relaxing" about the
need to reduce the scope of their plans.
Measures before Congress allowing HSAs to pay for certain nonpreventive
services on a predeductible basis could make CDHPs more attractive, Marcotte
observed. "Employers are interested in adding more flexibility so
high-deductible plans can cover value-based services outside the deductible,
such as chronic-condition management or care provided at centers of excellence,
and some proposals before Congress are beginning
to move in that direction."
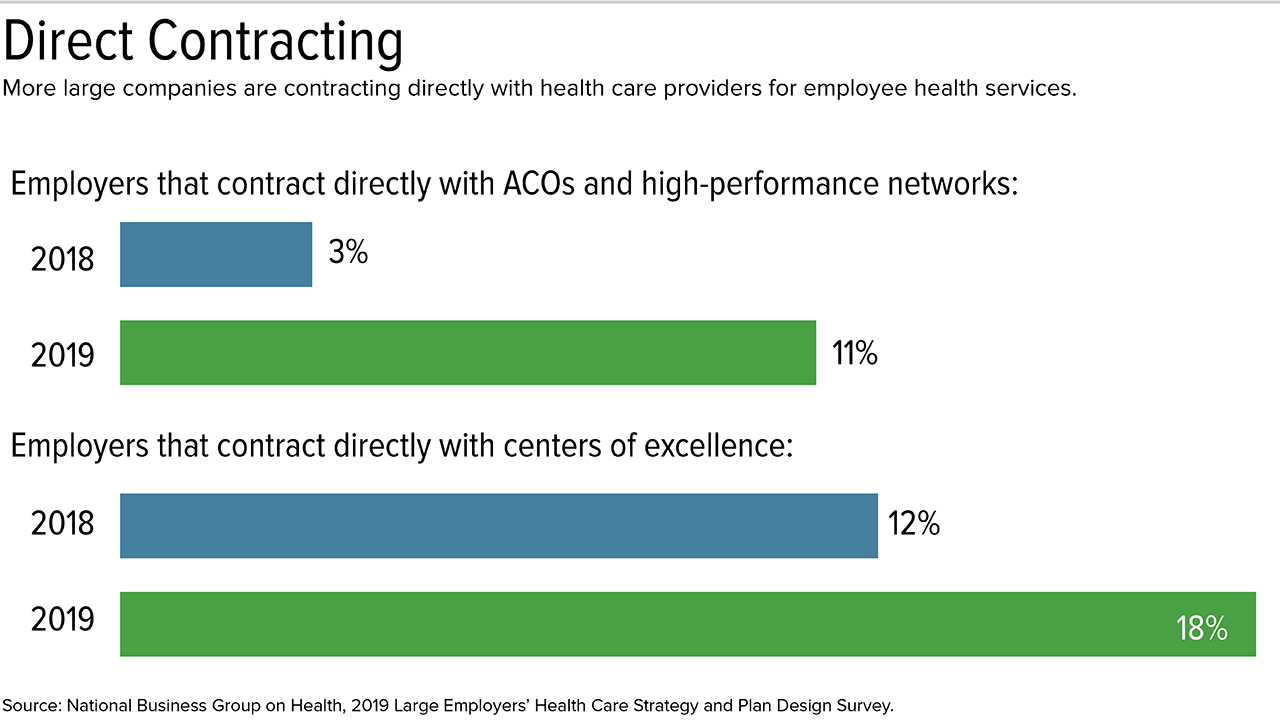
More large, self-insured employers are directly contracting for services with doctors and health systems. Direct contracting with accountable care organizations (ACOs) and high-performance networks jumped to 11 percent in 2019 from 3 percent in 2018, the survey showed. Direct contracting with centers of excellence (COEs) increased to 18 percent from 12 percent.
ACOs are groups of doctors, hospitals and other providers that come together
voluntarily to give coordinated, high-quality care to their patients.
High-performance networks limit in-network doctors, clinics and hospitals to
providers that are highly rated for cost and quality of care. Similarly, COEs
are highly rated facilities shown to offer high-quality, cost-effective care,
often focused on specific diseases or conditions.
While most direct contracting with COEs is with hospitals that specialize in orthopedics (i.e., knee, hip and spinal surgeries), direct contracting with cancer, cardiovascular and fertility COEs showed the greatest growth.
Employers are also contracting with medical facilities for comprehensive employee care. For example, General Motors recently negotiated lower costs with a Detroit-based hospital system to cover such wide-ranging services as doctor visits and surgical procedures for its local employees, the Detroit Free Press reported.
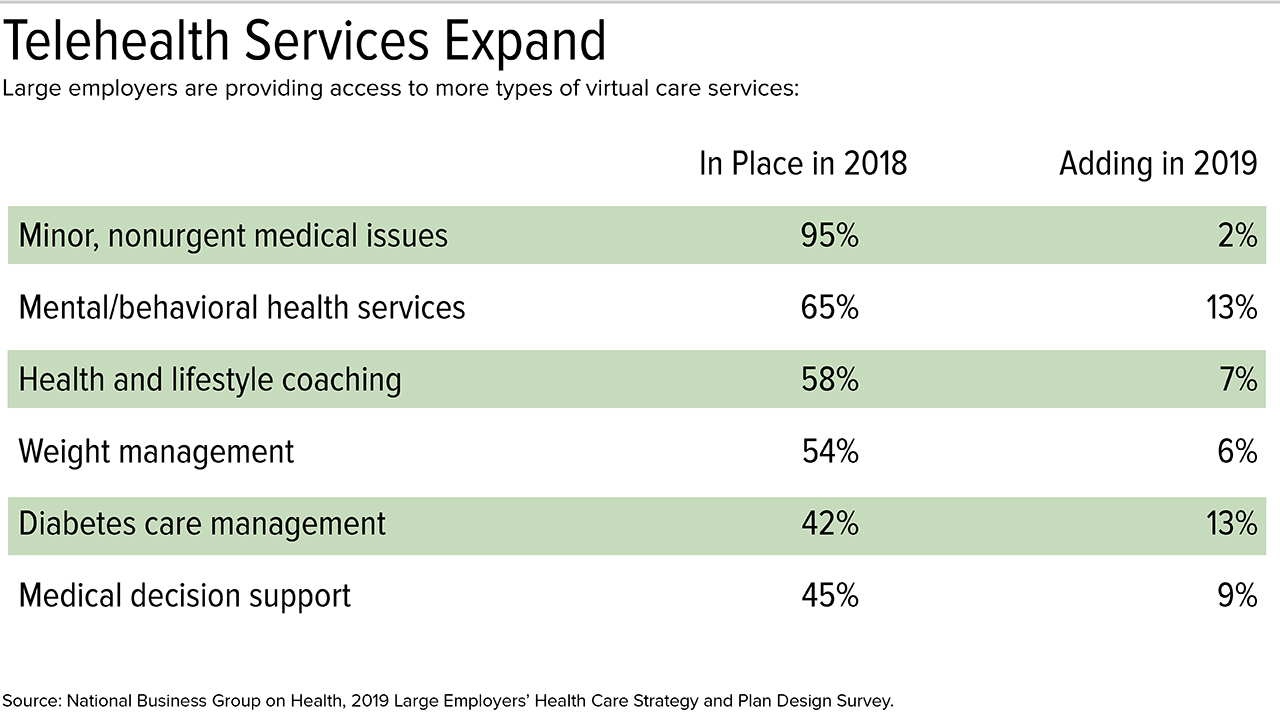
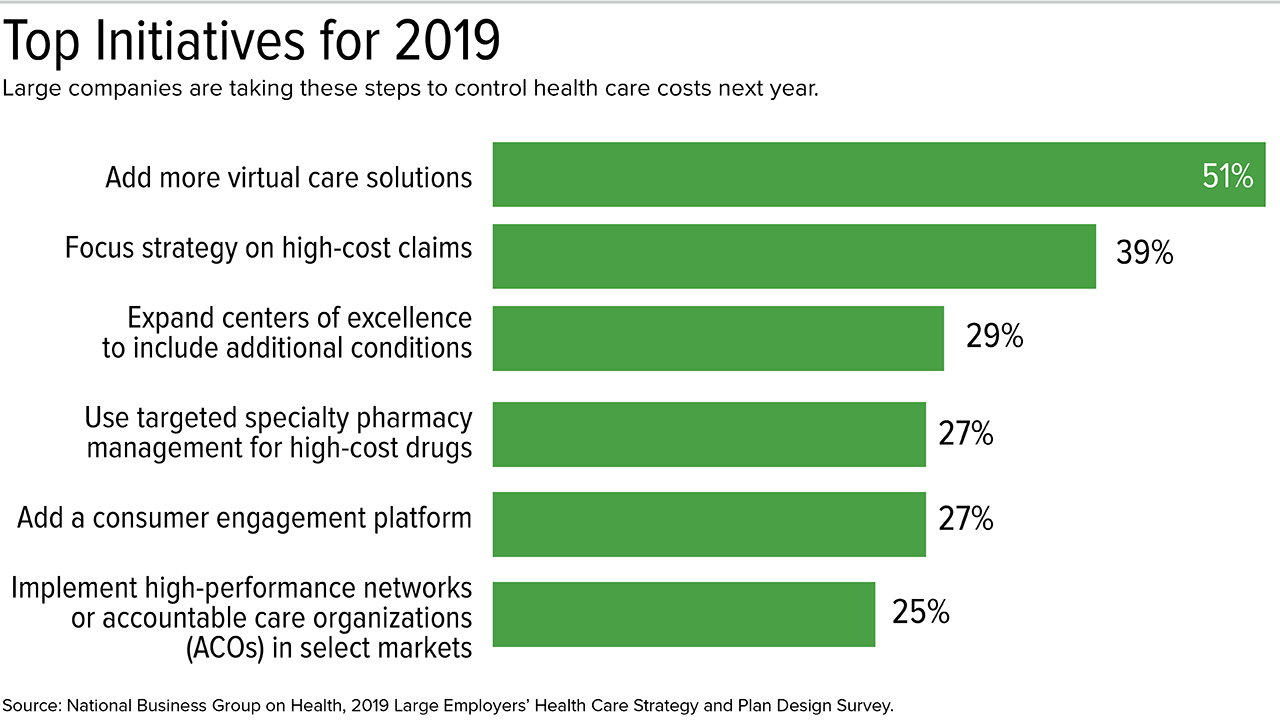
Nearly all large employers now provide telehealth or "virtual care" as an option for employees, and 20 percent of employers said the services are used annually by 8 percent or more of their workers. Just over half of respondents said their top health care initiative in 2019 was adding more virtual care solutions.
Telehealth has branched out well beyond physician consultations to include lifestyle coaching, management of chronic conditions such as diabetes, surgical decision support, physical therapy monitoring and cognitive/behavioral therapy, all of which show the greatest potential for growth over the next several years, the survey showed.
"The growth in virtual solutions largely reflects employer frustration with
the pace of change in how health care is delivered," Marcotte said. "Today, if
virtual care is not part of your health care strategy, your health care strategy
is not complete."
Specialty drugs are often "biologics" derived from living cells, and many are injected or infused intravenously. These expensive medications now account for 50 percent of most employers' prescription drug spending but are prescribed to just 1.5 percent to 2 percent of plan enrollees, Marcotte said.
In 2019, methods to manage specialty pharmaceuticals will include:
Three in four large employers do not believe drug manufacturer rebates are an effective tool for helping to drive down pharmaceutical costs, and more than half are concerned that rebates do not benefit consumers at the point of sale, the survey showed.
More companies are adopting a recently developed capability by PBM firms to make rebates available to consumers at the point of sale, rather than having the PBMs collect the rebates and pass the savings back to employers and health plans.
The survey found that:
Point-of-sale rebates, however, won't solve the problem of soaring drug costs, health care analysts say. "It would be better to have more reasonable pricing from the get-go and all along the line rather than discounts, rebates and other ways to adjust prices retroactively," Steve Wojcik, NBGH vice president for public policy, recently told Managed Healthcare Executive, a trade publication.
PBMs' tendency to include a drug on the plan formulary because the
manufacturer provides a rebate "leads to artificially inflated pricing and
greater costs for all consumers," Bob Marino, managing consultant at benefits
advisory firm OneDigital, told the publication.
Another challenge for employers is the growth of drug manufacturers' co-pay assistance programs for specific drugs, provided through discount coupons or medication-specific co-pay cards. Two concerns that employers have with these programs, Marcotte said, are that:
"To a health insurer, it looks like the consumer has paid for the drug and, as a result, the consumer's deductible and out-of-pocket payments for co-insurance are falsely satisfied," Marcotte said.
To prevent this, PBMs have developed the capability to track drug purchases
that received co-pay assistance, he explained. Next year, 29 percent of large
employers will have in place so-called "co-pay accumulator programs" that adjust
deductibles and out-of-pocket maximums downward to account for manufacturers'
subsidies, a number expected to grow to 50 percent by
2021.
Among other design trends noted in the survey are the continued use of
spousal surcharges, expansion of behavioral health benefits and actions to
address opioid addiction: